Homocysteine is an amino acid that occurs in the body as an intermediate in the metabolism of methionine and cysteine. Folic acid is a vitamin of the B complex, found especially in leafy green vegetables, liver and kidney. (Both these definitions are from the New Oxford American Dictionary on my MacBook.) Folic acid is B9, and folate is a salt of folic acid, but the two names are used interchangeably.
Homocysteine is normally broken down and recycled so that it doesn’t accumulate. This relies on sufficient amounts of vitamins B12, B6 and B9 being available to facilitate this process. Homocysteine, abbreviated Hcy, is a highly inflammatory substance associated with much higher risks of cardiovascular events. Research (AHJ 2004) has shown that it “causes endothelial dysfunction and damage, accelerates thrombin formation, inhibits native thrombolysis, promotes lipid peroxidation through free radical formation and induces vascular smooth muscle proliferation and monocyte chemotaxis.”
Naturally, we should strive to keep Hcy levels in our blood as low as naturally possible, which means around 6 micromol per litre. The higher its concentration, the worse off you are in terms of the potential for damage to the arteries and cardiovascular events. For a detailed look at Hcy in relation to vascular disease, read this article by Dr Neville Wilson (thanks Ivor Cummins).
Last week I explained something about Hcy, B12, and folate to my son who was getting ready to go back to university for his second year at St-Andrews. Afterwards, I thought it would be useful to share this with you, and I started working on this post.
This story is drawn from my own personal history. It is a case study with me as the primary subject using data I have collected from regular blood tests over these last seven years. However, I also use data from both my mother’s and my son’s blood test results that happen to be critical for understanding my own blood test results. Below, I describe the whole story and analysis of the data in detail. If you are not interested in the details, the punchline is this:
If your homocysteine levels are high, you should supplement with B12 and active folate in order to ensure the body has what it needs to process it. Some people lack the enzyme needed to activate the folic acid we get from food. This prevents the body from breaking down homocysteine that consequently accumulates in the blood. This is a genetically transmitted trait, which I think I have inherited and transmitted to my son. Because of it, we must supplement with activated folate to ensure breakdown of Hcy.
The first time I read about Hcy was many years in Anthony Colpo’s book The Great Cholesterol Con. The subject was discussed towards the end of the book in a short chapter, but I was left with a strong impression. Colpo emphasized that Hcy—unlike cholesterol—was a good predictor for heart disease. And it wasn’t just good: it was one of the best. But this wasn’t the only reason it made such an impression on me.
I read Colpo’s book after reading Uffe Ranvnskov’s Fat and Cholesterol are Good for You, and Malcom Kendrik’s The Great Cholesterol Con, both of which were about fat, cholesterol and heart disease, but neither of which discussed homocysteine. Then I read Gary Taubes’s Good Calories, Bad Calories, and again, Hcy wasn’t given the share of attention it seemed to deserve based on Colpo’s comments. If you’re new here, or if you need a refresher, you should read But what about cholesterol? and At the heart of heart disease.
The first time I got my Hcy levels checked was on August 27 in 2012. The result was 18.3 micromol per litre. On the results, the reference range was 5 to 15; moderately elevated was 15 to 30; and elevated was indicated as anything greater than 30 micromol per litre. Beside the middle range, it was written vitamin deficiency in parentheses. But it wasn’t written what vitamin deficiency would cause elevated Hcy. The doctor from whom I had requested the test didn’t know either. (As you might have experienced for yourself, most MDs don’t really know much when it comes to blood test results.)
I had already started supplementing with B12 by that time. Most of us, as vegetarians, quickly and usually angrily dismiss nutritional advice or warnings of potential problems from deficiencies that non-vegetarians love to offer when they find out we don’t eat meat. We usually interpret these as justifications of their feelings of guilt for not being vegetarians themselves. At least I know I did when I was vegetarian. Although most people who do give their unsolicited advice are rarely knowledgeable in the subject matter, I now know that I was dead wrong about my quick dismissal of several things in relation to dangerous deficiencies that come about when we eliminate meat and animal products from our diet. Vitamin B12 is surely the best example.
It was after reading this article on B12 by Mercola that I came to realize how disastrous were the consequences of living with low levels of B12, and in my case, how disastrous were the consequences of having been vegetarian for 20 years. I started supplementing right away, and got my first B12 blood test a few months later in 2010 on September 8. The result was 271 pg/ml. According to the lab who did the test, this was within range. But I knew it wasn’t. I knew this was much too low, and that I desperately needed to correct this as fast as possible, stop and hopefully reverse the neurological degradation associated with my long-standing B12 deficiency.
In that article was also underlined the connection between low B12 and high Hcy levels. It read: Cardiovascular and cerebrovascular diseases have a common risk factor – increased homocysteine levels in blood. Studies show insufficient amounts of folic acid and vitamin B12 can elevate your homocysteine levels, potentially increasing your risk for heart disease and stroke. So, of course I was worried. I was also angry at myself for having been so stupid and stubborn all these years… these 20 long years. But at least I now knew what I had to do: I needed to boost B12 levels and keep them high.
And I did. Look at how my B12 levels evolved over 7 years:

Blood B12 levels measured over seven years since September 2010.
Does seeing this make you wonder how the Hcy levels evolved? My expectation was that Hcy would drop as B12 rose. With some time delay of course, but still: as B12 levels increased, homocysteine concentration would decrease. Here is what happened:
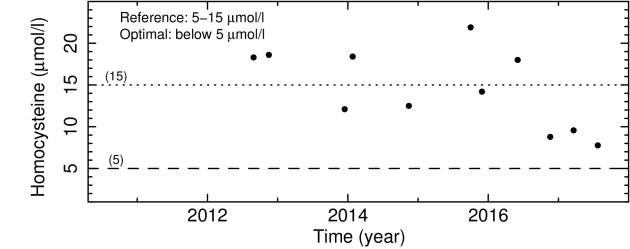
Blood homocysteine levels measured over five years since August 2012.
Not so obvious to interpret, right?
Let’s look at all the tests in which both B12 and Hcy were measured, and plot them one against the other. It’s called a correlation plot, and this is what we find:
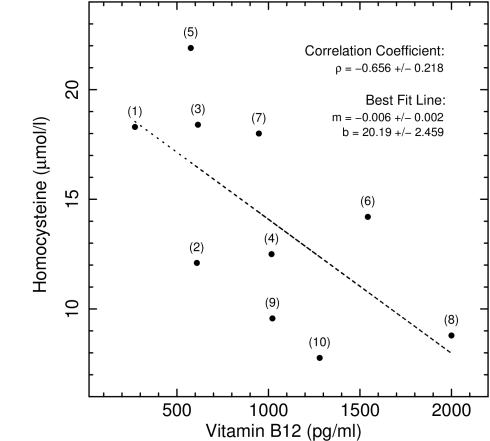
Homocysteine plotted against B12. Data point numbe labels show chronological order of tests.
So, there clearly is an inverse relationship between levels of Hcy and B12. There is no doubt in this. But at least for me, it’s not very tight. The correlation coefficient and the uncertainty on it quantify this relationship.
The coefficient can have any value between -1.0 and 1.0: a value of 1.0 signifies perfect correlation; a value of -1.0 signified perfect anti-correlation; and a value of 0 signifies that there is no correlation at all. The uncertainty on the coefficient quantifies how well the coefficient is determined from the data points, and therefore how loosely or tightly they are spread around the overall trend in the data set.
A coefficient of -0.66, as we found, tells us that there is indeed an anti-correlation in the relationship between Hcy and B12 concentrations. The uncertainty of 0.22 tells us that the correlation is not so tight. And when we look at two time series above, we see that although B12 has been above 600 pg/ml since 2014, Hcy levels remained more or less flat until the end of 2016.
My initial interpretation was that because I had been B12 deficient for basically 20 years, correcting that long-standing deficiency, and repairing the damage caused by it to the body and in particular to the nervous system, required maintaining consistently high levels of B12 for a long time, allowing the body the time needed to repair itself: two decades of B12 deficiency could obviously not be corrected in a few months. Maybe it was only after these 7 years of intensive B12 supplementation that the positive results were beginning to manifest themselves in this way.
And by intensive, I mean pretty serious. I started taking oral supplements of 2000 mcg per day; then transitioned to patches which are more effective because the B12 is absorbed directly through the skin without having to go through the digestive system; and finally moved on in early 2015 to monthly intramuscular injections of 5000 mcg of methycobalamin. Nevertheless, Hcy remained pretty much the same, even after months of injections. What was going on? Why wasn’t Hcy dropping?
Maybe you are thinking that there might be another way we could use to check how much influence B12 levels have on Hcy? Well, I have something I think is quite remarkable to share with you.
At the very end of July 2014, I brought my mother to a specialized blood analysis clinic, and ordered the complete set of tests listed on my essential blood test reference sheet. The results came back a few days later: her B12 was at 292 pg/ml; her folic acid was at 11.6 ng/ml; and her Hcy was at 30.5 micromol/l. She was 82 and, just for the record, it was the first time in her life that her B12 and Hcy levels had been measured in a blood test.
I immediately got a friend of hers and ex-nurse to give her methylcobalamin injections a couple of times a week. Five weeks later in early September we repeated the test for homocysteine. The result was 9.5!
My 82 year old mother’s homocysteine levels went from 30.5 to 9.5 micromol/l in 5 weeks following 10 injections of 1 mg doses of methylcobalamin B12.
She was out of the red. At least on that front. Hcy of 9.5 micromol/l is still moderately elevated when we consider that we would ideally have it around 6 or so. But 30.5 was dangerously high. This, to my mind, is strongly indicative of the crucial importance and immediate effect of vitamin B12 on homocysteine metabolism.
It wasn’t a tightly controlled experiment where everything was kept the same except the one variable under investigation, which in this case would have been the B12 injections. It wasn’t, because my mother did also at the same time adopt a new dietary regimen, following an alkalizing, very low carb, low protein, high fat, intermittent fasting cleansing protocol I had designed for her, that also included quite a number of other supplements. All were food supplements: vitamins A-D-K2, niacinamide, co-enzyme Q10 as ubiquinol, phospholipids as sunflower lecithin, omega-3s as krill oil, turmeric extract, tulsi extract, chlorella and spirulina, magnesium, zinc, iodine, etc.
Certainly it is true that everything influences everything else, but there’s no question in my mind that as far as homocysteine was concerned, the most important element in this protocol was the intramuscular injection of methylcobalamin approximately every three days. There is also no question that achieving such a drop in Hcy levels at such an advanced age and in so little time is nothing short of amazing.
The point of my retelling of this was to present direct evidence of the strength of the relationship between B12 levels and Hcy concentration. I think it does. Obviously, you are to draw your own conclusions.
Coming back to my case, in the fall of 2013, I stumbled upon The Complete Blood Test Blueprint in which Joseph Williams, a knowledgeable, experienced, and kind MD, was interviewed by Kevin Gianni, the host of Renegade Health, in a series of interviews that covered a large number of blood tests in great detail. I learned a lot things listening to Dr Williams. Admittedly, I was disappointed by the lipid panel discussion, and in particular by the discussion of cholesterol and lipoproteins. But putting this aside, I was generally very impressed.
Dr Williams talked about B12 deficiency at length, but I was already well versed in the subject by that time. I had recently read the book Could it be B12?, made detailed notes of it, and then posted for you B12: your life depends on it. Dr Williams also talked about Hcy. In that discussion was mention of the fact that in addition to B12 (cobalamin), B6 (pyridoxine) and particularly B9 (folic acid) were also essential for breaking down Hcy. I didn’t really think much of it, simply because my diet was and always had been rich in leafy greens, which naturally ensured a high intake of folic acid.
A few years and several blood tests later, I listened to the interviews again. And this time, something caught my attention in the part on homocysteine that hadn’t the first time: it was mentioned, in passing towards the end of the discussion, that some genetically predisposed people lacked the enzymes needed to activate folic acid; and that these people therefore needed to supplement with the already active form of B9 called tetrahydrofolic acid.
It caught my attention because by that time I had several measurements of Hcy that, even with my continued and even intensified B12 supplementation, were not showing evidence of going down. Remember: I started injections in early 2015. But there was something else that made this comment stand out for me: my son’s recent blood test results.
In July 2016 I brought my son to get a complete blood test that comprised all the markers I usually test for, together with all the major hormones, in order to have a baseline for him in his prime. It is certainly true that we can talk about optimal levels for each of the hormones we know and can test for. But our own personal ideal hormonal profile is unique to us. And the best time to get a baseline is when we are 18 years old: full grown adults at our youngest.
Laurent’s B12 was 578 pg/ml, his folic acid was 23 ng/ml, and his Hcy was 10.9 micromol/l. At 18, having had no major health issues, no accidents or serious diseases, a remarkably healthful fresh, green, organic, low carb, high fat diet of unprocessed whole foods for most of his life, I thought that this slightly elevated Hcy could be due to one of three things: either his body was still B12 deficient and just slowly building up its B12 stores, even though the three of us had all started with supplementation and patches at the same time; he was one of these people Dr Williams had made reference to who lacked the enzyme to activate folate, and therefore couldn’t effectively break down Hcy; or both.
I immediately ordered activated folate for us, and we started taking it in August 2016. If you take a look at the second plot that shows my Hcy levels as a function of time, you can see that it was just around 18 micromol/l at the end of July. And half a year later, towards the end of 2016, it was at the lowest it had ever been. Obviously, I was very happy to see this major improvement in achieving a drop in Hcy, something I had been trying to do for so many years. Therefore, also obviously, I continued taking activated folate. As you can see from the next two data points in 2017, Hcy was measured at 10 and then 8 micromol/l. We haven’t made another blood test to check Laurent’s levels. We’ll do that around Christmas at the end of this year when he comes back for the holidays.
Can we see how strong the relation between folate and Hcy actually is? We can plot the measurements we have one against the other like we did above for B12 and Hcy. What we find is this:
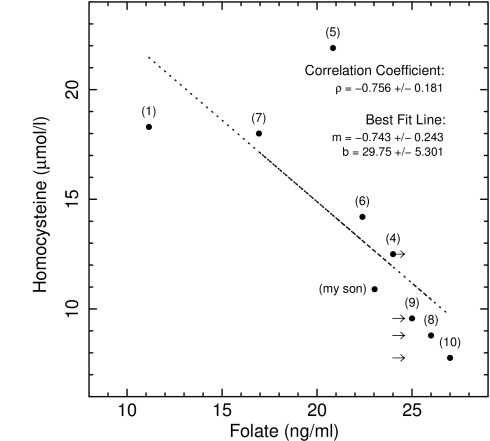
Homocysteine plotted against folate. Data point number labels show chronological order of tests. Arrows mark upper limits.
The relationship is very clear and linear. But I have to admit that I have cheated your eye a little bit. The measurements of folic acid are capped at 24: any value above that is simply reported as greater than 24. This was the case in tests (4), (8), (9), and (10). I show this with little arrows pointing towards higher values. Because the last three measurements were so close together in time, for the sake of clarity in the plot, I placed them at 25, 26 and 27, inversely proportional to the Hcy level. This is why they appear to follow the line. Otherwise, they would be at on the left edge of the arrows, one on top of the other, aligned with point (4), all at 24 on the x-axis. Note that I also plotted my son’s results (labelled as such), adding a data point at (23, 11).
What can we conclude from this investigation? Well, it isn’t totally clear cut and straight forward. I admit. But let’s review the facts:
For me:
- I was 38 years old at the time of my first B12 test.
- My B12 levels were low for 20 years: 270 pg/ml when first tested after few months of supplementation.
- My Hcy levels were high at 18 micromol/l about two years after starting B12 supplementation.
- B12 is necessary to break down Hcy.
- It took me 3 years of oral and patch B12 supplementation to reach 600 pg/ml.
- In early 2015 I started monthly B12 injections.
- Only after almost 2 years of injections did my Hcy levels drop below 10 micromol/l.
- But this precipitous drop in Hcy was concurrent with the start of supplementation with activated folic acid.
For my mother:
- She was 82 years old at the time of her first B12 test.
- Her Hcy levels were very high at 30 micromol/l.
- Her B12 levels were low for who knows how long: 292 pg/ml when first tested.
- She received approximately 10 injections of 1 mg in five weeks.
- Her homocysteine levels dropped from 30 to 9.5 micromol/l.
For my son:
- He was 18 years old at the time of his first B12 test.
- His homocysteine levels were moderately high at 11 micromol/l.
- His B12 levels were 578 pg/ml.
In addition to this, we have the plots above that show inverse relationships both between Hcy and B12, and between Hcy and folic acid. From this, there are at least three very clear conclusions we can draw:
- Low levels of B12 are associated with high levels of homocysteine,
- Higher levels of B12 are associated with lower levels of homocysteine, and
- Raising B12 levels leads to a decrease in homocysteine concentration.
At this stage and with the data we currently have, going further is more speculative. But here is what I think:
- I am one of these people that lacks the enzymes to activate folic acid.
- I might have inherited this trait from my mother, or much more likely from my dad, considering how well she responded to intensive B12 therapy. This was most likely also transmitted to my son.
- I was B12 deficient, and correcting this deficiency didn’t lower my Hcy levels.
- It was only when I started taking activated folate supplements that Hcy levels dropped quickly and significantly.
The reason I think this comes from two lines of reasoning. The first is that, as I just mentioned, it is only when I started taking activated folate that my Hcy levels dropped below 10 for the first time in seven years since the start of B12 supplementation.
The second is that even though both my mother and I were definitely B12 deficient, both probably for a long time, and that this would necessarily have led to an accumulation of Hcy in the blood that would have been greater in her case than in mine due to her age; my son was only 18 years old, and could not have been B12 deficient, at least not for almost 10 years. Nevertheless his Hcy levels were moderately elevated.
This is what I told him the other day. It took me only 5 minutes to tell him; it has taken me a lot longer to write this post. But I think the details are important if we are to understand things well. And by this I mean know what we understand, and know what we do not understand; know what conclusions we can make, and know what is hypothesis or speculation.
It’s not possible to be sure at this stage. We need more data and more experiments. But it’s not easy to gather such data, just because it takes a long time and strong commitments to be consistent with a supplementation programme over months and often years. If you have similar data and are willing to share, I would be happy to take a look at them.
Data like these trace and reveal so much about what’s happening inside our body, below the skin, far deeper than our eyes can see. But we can only begin to understand these measurements and the processes that drive their evolution by spending the time to look at them in detail. This is what we did here together. I hope you found it interesting.
Do you know what are your blood levels of homocysteine, B12, and folate? If not, you better get that checked out.
Become a proud sponsor of healthfully! Join our patrons today!
