Everybody knows that cancer rates are rising everywhere and every year. Everybody also knows that the words, “You have cancer. I am sorry.”, fall upon us like a death sentence. Everybody knows this, because we see it all around us, everywhere we look, and we hear about it every day, everywhere we turn.
If a doctor has, indeed, said these words to us, then we are probably scared, probably very scared. We know that basically everyone we have ever heard of who were diagnosed with cancer, died. Sometimes they died really quickly, like, within a few weeks. Sometimes they died within a few months. Sometimes it wasn’t so quick. Maybe it took a year of two, or three, or even five. They went through rounds of chemo. They were on sick leave at home for months on end. They sometimes appeared to recover at some point, maybe a bit, for a little while, but in the end, they died. And they died of cancer.
We also know that not even the most famous and richest people, like Steve Jobs, for example, can escape this kiss of death that the diagnosis of cancer delivers. Wealth and power are irrelevant when it comes to our prognosis as cancer patients: it is always bad. Of course, how bad it is depends on the kind of cancer, but why is it that so many different people, in so many different places, die of cancer every day?
I won’t venture into formulating an answer to this question, and I won’t dwell on cancer survival statistics. I don’t think it’s useful for us right now. I want to hurry and move to the good news. And the good news is that there many things you can do to help your body rid itself of cancer, which is usually the result of a long-standing disease process that has evolved over a lifetime, and has finally manifested itself in this way. This presentation of the question at hand is definitely not exhaustive, nor attempting to be. But this is what I consider to be some of the essential elements.

White blood cells (shown in blue) attacking cancer cells (shown in red).
Understanding cancer
To understand cancer, we have to understand the origin of cancer cells. Cells become cancerous due to a defect in energy production, a mitochondrial dysfunction, an inability to manufacture enough ATP (adenosine triphosphate) through oxidation of glucose or fatty acids to sustain the cell’s functions. This forces the cell to fall back on anaerobic (without oxygen) fermentation of glucose to supplement the deficient energy production from the dysfunctional or reduced number of mitochondria. Fermentation produces an increase in lactic acid in and around the cell. This decreases the availability of oxygen to the mitochondria, which further impedes their ability to produce ATP through oxidation of nutrients, and creates a negative feedback loop that pushes towards further mitochondrial stress and dysfunction, less oxidation, more fermentation, more acid, and less available oxygen.
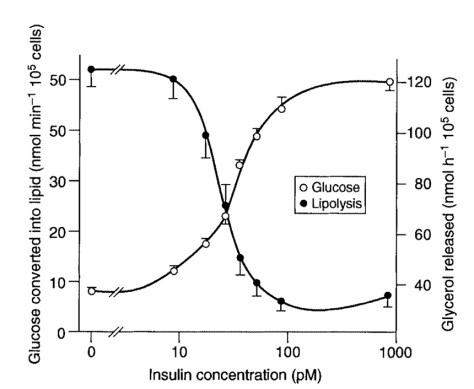
Because energy production through fermentation is so very inefficient, the cell needs far more glucose, and naturally develops more insulin receptors in order to be ever more sensitive to, and able to capture circulating glucose more effectively. Cancer cells often have 10 times more insulin receptors than healthy cells. What should be clear is that it doesn’t matter where the cancer is, and it doesn’t matter how it evolved, whether it was due to a gradual evolution from an environment too high in glucose, lacking in oxygen, and saturated with acid, or whether it was due to exposure to a toxin or mitochondrial poison, of which there are many and increasingly more in our environment. In the final analysis, this is how cancer cells become how they are, and this is how they survive.
As to their multiplication and proliferation from a single or small group of microscopic cells to large macroscopic tumours in one spot or all over the place, this can be understood by considering that the cell that is devolving from its normal function to that of cell whose only function is to ferment glucose at the fastest possible rate, loses, little by little, the ability to do whatever it was doing before, by losing the ability to produce ATP that can be used by its different specialised parts and constituents to perform their specialised functions, the cell becomes less and less specialised, less and less differentiated and therefore more and more general and more and more primitive, to the point where the essential ability of the cell to destroy itself, when something in its workings has gone wrong, is lost. Having lost this safeguard, the primitive, the undifferentiated, but also necessarily abnormal and weakened cell, just ferments and multiplies, limited only by its ability to fuel itself and sustain this most basic activity of survival without other purpose but this survival in and of itself.
Removing cancer
Having recognised and understood this, the strategy by which we can help the body rid itself of the cancer cells, and regain its healthy physiological functions becomes clear. We have to 1) do all we can to cut off the source of fuel to the cancer cells, 2) clear out the accumulated acids and transform the acidic environment into one that is alkaline and oxygen-rich, 3) help restore the cells’ mechanism of apoptosis—their ability to self-destruct, and 4) do everything else we can to further weaken and destroy cancer cells by means that simultaneously strengthen healthy cells. It’s a simple strategy that is also simple to put into practice, as we will see in a moment.
1) Starve the cancer cells
The first point is to cut off the fuel to the cancer cells. The source of fuel is glucose, because cancer cells can only ferment and cannot oxidise, and the way the glucose is supplied to the cell is by the action of insulin that moves it across the cell membrane. Therefore, what has to be done to is minimise the availability of glucose, and, more important still, minimise the availability of insulin to shuttle the glucose into the cells. The lower the glucose, the less potential fuel there will be. The lower the insulin, the less glucose will actually be able to enter cells. There is no real lower limit. Without ingesting any carbohydrates, the body maintains and regulates blood sugar according to the stress levels and kinds of activities we engage in, independently of how low insulin levels are. And so, the focus should be to have the lowest possible insulin levels naturally.
The fastest way to lower blood sugar, but especially insulin, is to fast, to stop eating altogether, and just drink water and herbal tea, remembering to eat enough salt to match the water intake. The second best way of doing this is in form very similar, but turns out to be much easier to do, is also a kind of water fasting, but with the addition of fat from coconut oil and butter, melted in the herbal teas. Both of these forms of fasting will most effectively deprive the body of anything that can easily be made into glucose, and of anything that will stimulate the secretion of insulin, thereby will allow glucose to drop as low as possible, but more importantly, insulin to drop and stay at an absolute minimum, and therefore most effectively starving cancer cells, no matter where they are in the body and bodily fluids, in the tissues and organs. The first form of the classic water fast is harder, but many people do it without hesitation nor difficulty. The second form is much easier, and may even be more effective in inducing a deep state of ketosis given the additional intake of medium chain fatty acids.
We can easily imagine doing such a fat “fast” for days, or even weeks, depending on the severity of the situation, our resolve to suffocate and starve the cancer cells as quickly as possible, and, of course, the state and circumstances in which we find ourselves. In addition, we can do this as much as possible on any given day, independently of what else we eat. The more fat and the less carbohydrate we ingest, the lower the insulin and the more effective the anti-cancer healing protocol will be.
The third option is to eat and drink to keep insulin levels as low as possible. Here again, because fat is the macronutrient that stimulates the least secretion of insulin, truly minimal, it should be the main source of calories. Simple carbohydrates and starches are most insulinogenic, and protein is about half as insulinogenic as are carbs. Indigestible fibre does not stimulate insulin. Therefore, in the extreme, we would eat only fat, pure fat. The best ones being the most natural and least processed, most saturated and least unsaturated: coconut fat, butter, animal fat and, the best of the vegetable oils, cold pressed olive oil.
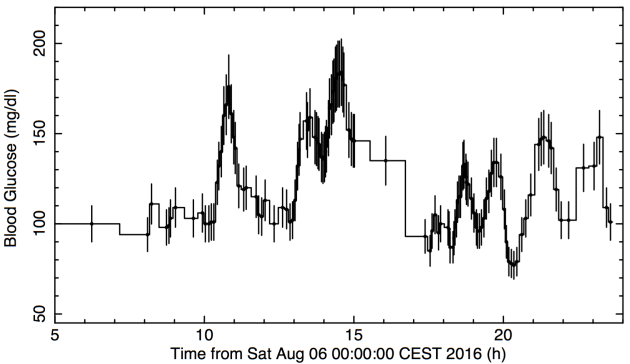
It’s important to understand the difference between having low blood sugar, and having low insulin levels. The first is like the amount of food in the kitchens of the restaurant, the second is like the waiter bringing it to the table. It is far, far more important in our efforts to stop the supply to cancer cells that we keep insulin levels as low as possible, than it is to try to keep glucose levels low. And to push the point further, it doesn’t really matter what the amount of glucose actually is, because as long as insulin is low, it will not be brought into the cell, into the cancer cells. The reason I emphasise this is because lack of sleep, emotional or psychological stress, intense physical exercise will all raise blood sugar levels temporarily, in some instances, to high levels. But as long as insulin is as low as it can be, the sugar will not be readily transported into the cells.
Naturally, we cannot have zero insulin, because we would die: our cells would literally starve to death, no matter how much we ate. Babies with a genetic defect that makes their pancreas not able to produce insulin always died of emancipation before the discovery and subsequent commercialisation of insulin as medicine. Similarly, if at any point in a child’s or adult person’s life, insulin stops being produced, incredible weakness and emancipation will follow, before it is tested and identified as the cause of their problem, hopefully in time before permanent damage ensues. Therefore, there is always some insulin in circulation, and therefore, sugar will eventually make its way into at least some cancer cells. This is why it is important to keep it as low as we possibly can naturally, and this is how we can appreciate the essential difference between the effects of high glucose and high insulin.
In a less extreme form than the fat-fast, we maintain low sugar and low insulin by getting and deriving most of our energy from fat. Eating cucumber or celery with almond butter or tahini, for example, or a green leafy salad with lots of olive oil, walnuts, and avocado, provides basically all calories from the fat, given that cucumber, celery and lettuce greens, are basically just water and indigestible fibre, while almond butter and tahini are 80\% fat by calories, and walnuts are 84\%. So is coconut milk, for example, at nearly 90\%, and dark 85\% chocolate, at 84\% fat based on calories. Focusing on feeding the body with these kinds of healthful, high-fat foods, will nourish, stimulate healing, and keep insulin and glucose levels as low as we can without either water fasting, or consuming only fat.
2) Alkalise to remove and excrete accumulated acids
The second point is just as important as the first, because it is the environment in which the cells live that actually has the most direct effect on their function. We have looked at the importance of achieving and maintaining an alkaline environment in the body in several other places. The essence is excellent hydration with alkaline water (pH>8) combined with the intake of proportional amounts of unrefined salt to promote the release of acids from the tissues, and its excretion through the urine by the kidneys. Without proper hydration, the cells will retain the acid with the little water they have to hold on to. Without proper amounts of salt, the kidneys will also retain the acid in order to maintain the concentration gradient that allows the nephron to function when it re-absorbs water.
Naturally, alkaline water will work infinitely more effectively. But the most important detail is the controlled balance between water and salt intake, and what we want is a lot of water and a lot of salt. We cannot take in large amounts of salt water without getting loose stools. So, it has to be smoothly distributed throughout the day, except in the morning, when we get up, because we are dehydrated, and need to drink about 1 litre of water over the course of one to two hours, before we start taking salt.
If you buy mineral or spring water, find the one that has the highest pH value. It should be greater than at least 8. If you have a water filter at home, then add alkalising drops to it before drinking it. I use Dr. Young’s PuripHy drops.
As acidity decreases, and the environment becomes more alkaline, oxygen will flow more freely, and become more available to mitochondria for oxidising fatty acids in producing energy. Remember that cancer cells do not use oxygen, and cannot use fatty acids to fuel themselves, whereas normal, healthy cells, not only can, but function much more efficiently on fat rather than glucose as their primary fuel. Adding chlorophyll and fresh juice of green vegetables to the alkaline water is an excellent way to further boost alkalisation, neutralisation, and elimination of accumulated metabolic acids. Unlike the first step, which is to lower insulin and glucose levels, and that can be done, to a great extent, literally overnight under fasting conditions, alkalising to eliminate accumulated acids is something that takes time. But in both cases, what matters most is consistency. Hour by hour, and day after day, the body will do what it needs to do as best is can, and improve in these functions with time.
Beyond this fundamental necessity to hydrate with alkaline water throughout the day, and day after day, the most therapeutic way to alkalise the tissues, and detoxify the body, is by taking medicinal baths in which we add two cups of sodium bicarbonate (baking soda), and two cups of magnesium chloride (nigari), or magnesium sulphate (epsom salts), if nigari is not available. This is easy, relaxing, extremely medicinal, and very effective in neutralising and eliminating acids and toxins from the body. In fighting cancer, you should be soaking in this kind of hot bath for 45-60 minutes three times per week. The benefits of this ultra simple trans-dermal therapy with sodium bicarbonate and magnesium are incredible. You can read a lot more about this from the baking soda, magnesium and iodine doctor, Dr Sircus.
3) Restore cellular self-destruct function
The third line of action is also essential, and it only requires you to take a few key supplements. The most important of these in the fight agains cancer is iodine, because of its fundamental role both in the structure and architecture of cells, but also in the regulation of apoptosis, the process by which a damaged cell will self-destruct when things have gone wrong somewhere. The importance of iodine cannot be overemphasised. And in healing cancer, or any serious disease condition, we will want to take high doses daily. Doses of at least 50 mg, but preferably 100 mg.
However, because of its very strong detoxification effects, as it pushes out all accumulated toxic halogens out of the cells to replace these by iodine in its proper place, we must work up to these high doses gradually, starting with 12.5 mg, and increasing the dosage as quickly as possible given the body’s response to it. Some people , maybe most, will experience headaches and possible nausea when starting on iodine. This is perfectly normal. The stronger the reaction, the more indicative of the body’s level of toxicity. Therefore, you should always view this as something good, in that toxins are being excreted out of your cells. It is important to support the detoxification process by taking chlorella and spirulina, probiotics and psyllium husks every day as well, while always drinking a lot of alkaline water with added chlorophyll for extra cleansing, if possible.
What I take and consider to be the best supplement is Iodoral by Optimox. Optimox recommends taking the iodine on an empty stomach for faster absorption, but it can also be taken with food for slower and possibly better assimilation. In addition, although iodine can easily be taken on an empty stomach, the co-factors, which include B vitamins, are much better taken with food to avoid potential nausea or queasiness. Moreover, taking it with food will slow down the absorption, and thereby decrease the negative sensations from the detoxification effects. The only thing is that iodine, given its stimulation of thyroid function, will energise the body. Therefore, it should be taken before midday. I take it either first thing in the morning or at lunch (or both).
You can read about the importance and functions of iodine in the following three books: Iodine, Why You Need It, Why You Can’t Live Without It by Dr. Brownstein; What Doctors Fail to Tell You About Iodine and Your Thyroid by Dr. Thompson; and The iodine crisis: what you don’t know about iodine can wreck your life by L. Farrow. There are also many web resources and highly informative forums about iodine and cancer. You can search for the words iodine and cancer to see for yourself.
Other fundamentally important micronutrients are vitamins B12 and D, both of which are needed for proper cellular function, and DNA transcription and replication, because of their roles in the nucleus of cells, activating and de-activating, switching on and off genes, to ensure everything in the cell works as it should. For best and fastest results—and that’s definitely what we need in our fighting cancer—B12 should be injected weekly in the amount of 1 mg, and in the form of methylcobalamin. (For optimal health in normal circumstances, it can be injected once a month in the amount of 5 mg.) Vitamin D should be taken with its sister vitamins, A and K2, for synergistic effects and biochemical balance in their functions. Each of these have complimentary roles, and should generally be taken together, unless there is a reason not to. You can read these two articles published by Chris Masterjohn from the Weston A. Price Foundation to learn why and how: On the trail of the elusive X-factor: a sixty two year old mystery finally solved, and Update on vitamins A and D.
It is by supporting proper cellular function, especially in the nucleus, with iodine, B12 and D, that cells will regain, little by little, the ability to recognise that they are damaged and need to self-destruct. There will always be millions or even billions of cells involved in the disease process we call cancer, but they will be distributed along a wide spectrum of dysfunction, from having very mildly impaired mitochondrial function from a light oxygen deficit cause by a little too much acid in the environment surrounding the cell, to full cancer cells that derive 100% of their energy needs from anaerobic fermentation without using any oxygen at all, and thriving in extremely acidic conditions.
Hence, many cells will die from being starved of glucose, because that’s the only fuel they can use; many cells will recover enough of their normal regulatory mechanisms to know its time to self-destruct; and many cells will actually regain their healthy function, repair their damaged parts, and replace their dysfunctional mitochondria with new ones. Nothing is ever black and white when it comes to cells and cellular function. Instead, everything is grey. But it is a million different shades of grey.
4) Do everything else that can help
The fact is that there are many, many more things you can do. Many therapies, many treatments, many supplements and herbal formulas, that have all proved highly effective against cancer. There are so many that many books have been written about them: About Raymond Rife, you can read The Cancer Cure That Worked by Barry Lynes; about Gaston Naessens, you can read The Persecution and Trial of Gaston Naessens: The True Story of the Efforts to Suppress an Alternative Treatment for Cancer, AIDS, and Other Immunologically Based Diseases by Christopher Bird; about Rene Caisse and the Essiac tonic, you can read Essiac: The Secrets of Rene Caisse’s Herbal Pharmacy; about Johanna Budwig, you can read Cancer – The Problem and the Solution; and the list goes on. There are websites devoted to these people and their approach to cancer, and this is just a few of them that I know about. One book that compiles a lot, maybe most, of the information on non-toxic treatments for cancer, is Ty Bollinger’s Cancer: Step Outside the Box.
Maybe you find it hard to believe that our governmental and medical authorities would have gone—and continue to this day—to go through such extreme measures in order to suppress treatments that work so effectively to help and heal people of their illnesses and of cancer, without negative side effects, and at very low costs. But this is a simple fact. And it is quite easy to understand if we consider that anyone, or any institution, that has commercial investments and interests in a particular endeavour, will go to great lengths to maintain and strengthen, as much as they can and for as long as they can, the conditions that make them successful. There’s nothing more to it than that. Let’s look at a few of those therapies and supplements which are easy to implement, and highly effective against cancer: hyperthermia, flax seed oil, enzymes, and turmeric.
Hyperthermia, or heat therapy, is a very well studied and effective therapy against cancer, both preventatively and curatively. The idea or principle is very simple: healthy cells can withstand high temperatures without damage. The reason why this is so, and why we know it for sure, is that the body produces fevers as a defence mechanism to destroy invading viruses and bacteria that, unlike our own cells, cannot withstand the heat. Similarly, cancer, and other compromised and damaged cells, are unable to cope with high heat. Hence, it was hypothesised, tested, verified and demonstrated that hyperthermia is really very effective at destroying cancer, while simultaneously cleansing and strengthening healthy cells and tissues. Infrared saunas are ideal in heating the tissues more deeply, but any sauna, steam room, or even bath that induces hyperthermia by raising the temperature in the body, will help kill cancer cells, cleanse, and restore health.
Enzyme therapy has also been used for many decades in the treatment of cancer patients extremely successfully. The late Nicolas Gonzalez who passed away last year, was its most recent champion, following in the footsteps of his mentor, Dr William Kelley. The treatment protocols are more complicated, and are always highly individualised, but the main element is the supplementation with large doses of enzymes, combined with the colon cleansing to eliminate the dead tumour tissues from the body. Large quantities of fresh vegetable juice are also often included in his recommendations. You can read about it here: http://www.dr-gonzalez.com/index.htm, but whether you decide to throw yourself completely into it or not, I strongly recommend taking proteolytic enzymes three times per day, always on an empty stomach at least 30 minutes before eating, and support cleansing by taking a colon cleanser before going to bed. This site, http://www.losethebackpain.com, has good quality enzymes and cleansing supplements that we’ve used, but you can also do your own research.
Flax seed oil, organic and cold pressed, combined with fresh organic quark or cottage cheese is, based on Johanna Budwig’s extensive, lifelong research, as well as practical clinical experience with patients, is another one of the most effective and simple cancer treatments. And although the biochemistry of it, and biochemical pathways through which the cancer is weakened and destroyed may be complicated, the implementation is very easy and simple, costs very little, and cannot in any way bring about harm, unless one is severely allergic to milk proteins (in which case the dairy can be replaced with another source of protein that will work as the carrier). Here is a good article that has links to other excellent articles about this: https://www.cancertutor.com/make_budwig/
Turmeric, an ancient, bright yellow, Indian spice, which is a powder made from drying the ginger-like root that is turmeric, is one of the most researched natural substances in modern times, and is surely one of the most powerful natural anti-cancer supplements. Since it has tons of wide-ranging health benefits, and carries no risks at all, it’s clear that everyone can benefit from it. You can read about it from Mercola here. You should take it three times per day, but with your meals, because the more fat there is in the gut, the better the absorption will be, as is true for most antioxidants, vitamins, and minerals.
I feel it is important to emphasise the point just made about the risk-free nature of supplementing with turmeric, because it is a crucial point that applies to everything we have discussed here, and everything we have discussed in all the natural healing protocols and nutritional approaches we have presented in the past. Food-based nutritional healing is, in general, risk-free, because it doesn’t involve ingestion of or exposure to toxic substances, and instead involves correcting deficiencies, boosting nutritional status, and optimising the biochemical and hormonal environment of the body in order to promote healing.
Of course, we can object by referring to examples of people dying from drinking too much water too quickly. But we are not talking about such extremes. Nonetheless, we could, for example, eat coconut oil or butter all day, and other than the possible nausea from taking in so much fat, you wouldn’t get anything more than loose stools. Moreover, the body’s own hormonal responses would naturally prevent overconsumption through a feeling of extreme satiety that would basically make it impossible to willingly eat more.
Another example is that of using baking soda or iodine. So simple, and yet so powerful, they stand as the perfect examples of the benign nature but extreme effectiveness of natural healing. We find written in the most recent edition of the Manual for the Medical Management of Radiological Casualties of the US Military Medical Operations, Armed Forces Radiobiology Research Institute, that sodium bicarbonate will “prevent deposition of uranium carbonate complexes in the renal tubules”, and that we should, “within 4 hours of exposure, administer potassium iodide (KI) to block uptake of radioactive iodine by the thyroid”, because they are the best known ways to protect the kidneys and thyroid from being destroyed by the radioactive elements that would—without the use of sodium bicarbonate and potassium iodide—migrate to these organs and destroy them.
But why wait for a chemical spill or a nuclear power station meltdown in order to rid the body of accumulated chemicals and toxins, and to replenish every cell with a plentiful supply of iodine to ensure that all cells and all glands function at their best, now and every day? We don’t have to wait. The same goes for turmeric, for enzymes, for B12, for A-D-K2, for hydration, for alkalisation, for minimal glucose and minimal insulin loads, for maximum nutrition and maximum health. Why don’t we start doing this preventatively right now?
Summary and Wrap up
Maybe you know all of this stuff already, or maybe you don’t and you are blown away and overwhelmed by the amount of information and range of topics we have covered. Maybe you are reading this because you are interested and curious to learn and be as well-informed as you can about health topics, or maybe you are desperately looking for relevant information that can help you or a loved one. No matter in which camp you find yourself, here is the summary and wrap up I can offer to bring all of what we have discussed down to a simple set of recommendations that anyone faced with a diagnosis of cancer, and fearful of, or skeptical about, or doubtful that the current standard of care in the cancer industry will help them, can understand and follow, knowing that none of these food choices, supplements, and therapies will bring them harm in any way, and that all will only do good, regardless how dire or hopeless their situation may appear to be.
- Keep low insulin levels, as low as possible, by not having insulin-stimulating carbohydrates, and by keeping protein intake reasonably low. Focus on consuming natural, unprocessed fats as much as possible to supply the largest proportion of your daily calories. Consider a water or a tea-with-fat fast for a few days when it is suitable, or even as an intermittent fasting strategy on a daily basis. Consider also doing a green juice “fast” (only green vegetables) with added fat from blending in melted coconut oil or milk.
- Drink alkaline water, always on an empty stomach, considering the day as divided between hydration periods, and feeding and digestion periods. The first hydration period is from the time you get up until you have your first meal. It is good to extend that period if you can to allow plenty of time for proper hydration after a long night of dehydration, with at least 1 to 1.5 litres over a period of at least 2 hours. Drink slowly to improve absorption and not pee everything out. Always allow 30 minutes without drinking before meals, and 2-3 hours after meals, depending on their size. The cycles of hydration and feeding during the day (for 3 meals) should be as follows: drink, wait, eat, wait, drink, wait, eat, wait, drink, wait, eat. For only two meals, which I recommend, then periods of drinking are extended and allow for even better hydration, cleaning of the blood, and better digestion.
- Take iodine supplements with the co-factors and with food to maximise absorption and effectiveness. Start with 12.5 mg per day, and work your way up to 100 mg. Do this as quickly as your body allows you to. Take the iodine every weekday, and stop on weekends; five days on, two days off. (My wife and I take 50 mg per day.)
- Take hot baths with sodium bicarbonate and magnesium chloride (or sulphate; 2 cups of each). Soak for 40 to 60 minutes. Do this three times per week. Always take your baths on an empty stomach, and drink at least one litre of alkaline water during the length of the bath. (Once per week is what I aim for as preventative medicine.)
- Get B12 injections of methylcobalamin, 1 mg on a weekly basis. (My wife and I get a 5 mg injection once per month.)
- Take proteolytic enzymes and Essiac tonic three times per day, always on an empty stomach, always at least 30 minutes before meals. (We take it once, first thing in the morning.)
- Take turmeric and turmeric extract, as well as A-D-K2 with every meal or fatty snack, three times per day during recovery. (Once daily in normal circumstances.)
- Take infrared or regular saunas, every day if possible, or even in the morning and at night if you have or decide to buy your own little sauna. I would definitely do this given how effective hyperthermia is at destroying cancer cells.
- Eat Budwig cream.
- Eat and drink greens.
- Spend time outdoors, as much time as you can, moving, breathing fresh air, exposing your skin to the sunlight.
- Keep low stress levels, as low as possible. Take tulsi, ashwagandha, and HTP-5 to keep stress hormone levels low, and mood high.
- Take probiotics, chlorella and spirulina in the morning, and a colon cleansing supplement before bed.
- Sleep well, long restful nights. Melatonin is very useful for this, and has many additional health benefits.
Cancer is very easy to prevent, but somewhat harder to dislodge once it has taken hold somewhere within the body. But no matter what type of cancer, how localised or generalised it is, or at what stage it finds itself, there is always hope. Hope of getting better and more comfortable, and hope for a complete recovery.
We have to remember that cancer cells are degenerate and weak. By making the environment as health-promoting to normally functioning cells, and simultaneously as hostile as possible to cancer cells, they will perish and be cleared out from the body as the waste that they are. The body heals itself, often miraculously quickly, when impediments are removed, and the elements needed for healing are provided. With all my heart, I hope this can help you and your loved ones.
If you think this article could be useful to others, please ‘Like’ and ‘Share’ it.