A young man I know recently started to play rugby at a higher level, and thus more seriously than he ever has in the past. Being a smart guy, he wants to get his nutrition “on point”, as he writes, in order to perform at his best. He started reading about nutrition on the internet, and found it to be like “a snake oil convention”, which it most certainly is. So, he contacted me to get my opinion on the subject. I’ve been meaning to start writing about training and performance for a while, and balance out all my writings about disease and overcoming disease conditions, and so I thought this would be the perfect opportunity to start.
The first thing that needs to be said is that there are common aspects as well as differences in the way training and nutrition should be optimised for different disciplines and goals. In common to all disciplines, are that we always want to perform at our best, and recover as fast as possible. Those are the basic and most fundamental drivers.
Differences are much greater in number and far wider ranging in kind, but they can include core aspects like the duration of the event: speed and power versus endurance and stamina (think of the 100 meter dash versus the marathon, or the velodrome cyclist versus the Tour de France rider); the kind of effort required: sustained versus bursty (think of rowing versus tennis); the medium and nature of the forces against which we are working: water or air, with an intervening machine or without (think of swimming versus jumping towards the rim to slam dunk the basketball, skying versus bobsledding, wrestling or judo versus Formula 1 racing).
In every case, there are preferred and optimal skills and trained reactions, fitness and body composition, as well as morphology and muscular development. For now, let’s just look at the basics in the sense of what every athlete would want and would benefit from no matter what kind of activity they do: best performance and fastest recovery.
The most fundamental point is mitochondrial energy production
At the root of all activity of the body, and at all levels, is the generation of ATP by mitochondria. This is really the bottom line for everything, because this is what cells use to function and do what is required of them in every instant. Mitochondria, small organelles thought to have migrated into a cellular membrane early in the history of evolution of life on the planet, are present in every cell in different amounts, and are essential for life. They can oxidise or burn any macronutrient—glucose, amino acids, or fat—to produce ATP, but the bulk is derived either from glucose or fat. In the process, they produce byproducts of different kinds and in different amounts based on the nature of macronutrient used for fuel, and on the energy demands. Therefore, for optimal performance with a fixed number of mitochondria, we want:
- the maximum efficiency in ATP energy production, and
- the minimum amount of metabolically taxing byproducts.
These question of deriving the most amount of ATP in the most efficient way with the least amount of byproducts that ultimately impede physiological function, has been considered in On the origin of cancer cells (1 and 2). To summarise in very few words: fatty acids are the most efficient way to store energy, on a gram-per-gram basis they produce the most ATP when oxidised by the mitochondria in an oxygen-rich environment, and their oxidation result in the least amount of acidic and physiologically costly byproducts. Therefore, the inevitable and obvious conclusion, is that for optimal physical performance, we want maximum metabolic efficiency, and for maximum metabolic efficiency, we need to provide the conditions that allow our cells to use fatty acids as their primary source of fuel.
The key is efficient fat utilisation
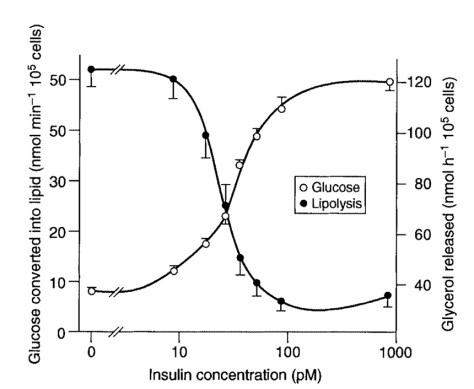
Efficient fat utilisation is achieved in three stages, which are really just two, because the second and third blend into one another seamlessly. The first step is making sure cells can use fat as fuel. Because insulin signals cells to store energy, it prevents fat utilisation (lipolysis). Inhibiting lipolysis is one of insulin’s main functions. To allow cells to burn fat, insulin must be low. To lower insulin levels, we must either fast, or restrict carbohydrates (and to a lesser extent protein). In fasting conditions, most people will reach insulin levels low enough to start fat-burning after 12 to 16 hours. With severe carbohydrate and protein restriction, that means getting all or almost all of your calories from fat, the timescale is probably similar.This first step is therefore achieved within 24 to 48 hours.
The second step is basic adaptation to deriving cellular energy needs from fatty acids, those that we eat, and those that are stored within the body’s fat cells (adipocytes). This is achieved over the course of about 4 weeks by maintaining a very low carbohydrate, low to moderate protein, and high fat diet.
The third and last step is full keto-adaptation, achieved within two to four months of consistent carbohydrate restriction. The word keto in the term keto-adaptation refers to the fact that, from the breakdown of fats, the liver manufactures ketones, the one we measure as a marker is usually beta-hydroxybutyrate, used primarily to fuel brain cells that can only use glucose and ketones. This stands in contrast to most other cells that can use fatty acids directly. An exception to this—the only one, as far as I know—are red blood cells that can only use glucose.
A point that needs to be appreciated relates to the potency of insulin to stop fat-burning. As soon as glucose spikes, insulin will spike, and will stop fat-burning. This is particularly important if we are aiming to burn as much fat as possible or become as efficient fat-burners as possible. Consequently, the very worst thing we can do is to have sugar in the morning, just before or just after training. Even a small piece of fruit will do it. This will generally always stop fat burning in its tracks. And not just for a few minutes, but for hours, all the hours necessary for insulin levels to drop back down low enough to allow lipolysis to start again.
Maximally efficient fat utilisation is where an athlete wants to be, because this will ensure that they always use as much fat and as little glucose as possible, maximising endurance potential while minimising production and accumulation of lactic acid in the muscles. The most important benefits this brings are to be able to sustain long hours of exercise without “hitting a wall” from the exhaustion of glycogen stores, and having muscle fibres that can function smoothly unimpeded by the presence of large amounts of lactic acid, something which also significantly accelerates recovery, as very little time is needed to clear out the small amounts that remain in the muscle after the event or training session.
Fat stores are, for practical purposes, inexhaustible. Even in very lean athletes (below 10% body fat), there will be between 5 and 10 kg of fat reserves to draw on during that ironman, that ultra-marathon, or that mountain-bike-around-the-clock event. Each gram of these 5-10 kg provides 9 kcal of fuel. And so, that endurance event lasting 12 hours during which you burn 7500 kcal could be fuelled with just 830 g of body fat. Naturally, this would not happen, because glycogen from the liver and the muscles will always be used in greater or lesser amounts depending on the level of stress (physiological and psychological), and intensity of the exercise. Nonetheless, this is a good illustration of the massive reservoir of fuel we have at our disposal if we train the body to utilise fat efficiently.

The Mont Blanc ultra-marathon. All long distance runners should be keto-adapted.
To get to this point, the muscle cells need to be trained to use fat, first at very low intensity to make sure that they can fuel the activity using mostly fat, and then gradually increasing the level of intensity to force adaptation in continuing to burn fat as the primary fuel. Best way to achieved this, is by doing low intensity endurance work in a fasted state. And over time, gradually extending duration and increasing intensity.
Moreover, doing intense, muscularly demanding, resistance training in the fasted state, is beneficial in many additional ways, including the secretion of greater amounts of growth hormone and testosterone for better growth and repair of tissues, as well as more effective fat utilisation, and protein recycling, which involves the breakdown of damaged, scarred, and otherwise unused tissues in order to maintain, feed and rebuild the muscle tissues that are being used. The same mechanisms involved in protein recycling, act to preserve muscles that are active, while facilitating the breakdown of other tissues, and in particular fat stores, that are not.
There are many benefits to training in a fasted state, and doing both low intensity endurance, as well as high intensity resistance training. This is especially true over the long term, as the body becomes increasingly more efficient at fat utilisation, increasingly better at preserving active muscle mass, and increasingly more effective in repairing damaged tissues and cleaning out metabolic wastes. Such conditions are naturally highly favourable for building strong, healthy, lean muscle mass.
Fast recovery requires minimising inflammation
Whenever we do anything physical, some level of micro tears, fractures, and injuries to the muscle and bone tissues take place. The body’s repair mechanisms involve an inflammatory response. Without a healthy inflammatory response, we would not be able to recover from injuries, recover from training, or build bone or muscle mass. In fact, we would not be able to survive. What we want, is a fast and effective inflammatory response to heal, repair, or build whatever needs fixing as quickly as possible. What we do not want is a low-level of chronic inflammation that cripples the body from functioning at its best.
One of the greatest advantages of running on a fat-based metabolism with maximally efficient fat utilisation, is the fact that the muscle cells are fuelled by burning fatty acids without producing lactic acid. This is in stark contrast to a glucose-based metabolism, where most of the energy is derived from burning glucose, and this always produces lactic acid. As intensity increases, the amount of lactic acid produced will depend first on the intensity, and second on the level of keto-adaptation. The better the keto-adaptation, the more fat will be used to fuel the cells at higher levels of intensity. But, no matter what, the keto-adapted individual, and the athlete in particular, will always, and in all circumstances, produce less lactic acid than the one running a glucose-fuelled metabolism.
All acidic metabolic waste products need to be eliminated from the body. This is the role of the kidneys, whose function we have explored in The kidney: evolutionary marvel. For lactic acid that accumulates in the muscles, the first stage is to get it out of the muscle, and this usually takes quite a while. It can take from hours up to several days. The process of clearing it out can be accelerated using massage, stretching, and very low intensity exercise. Alkalising baths are a fantastic therapy for accelerating recovery, and lowering inflammation. Magnesium chloride and sodium bicarbonate baths are therefore an absolute must for the serious athlete. We have detailed the importance, roles and functions of magnesium in Why you should start taking magnesium today, and discussed inflammation and the importance of alkalisation in Treating arthritis (1 and 2).
In the end, all metabolic acids lead to increased inflammation, and, when they accumulate in joints and tendons, inevitably to injury. Insulin-stimulating carbohydrates also cause inflammation. They trigger hundreds of inflammatory pathways. And so, by eliminating them from our diet, and allowing the metabolism to run on fat, we have done as much as we could ever do with our food to minimise inflammation in the body. This is what an athlete wants for the fastest possible recovery time, with best training performance, and the smallest risk of injury.
The final and most important element for fast recovery and low inflammation is optimal hydration. This is the most important because all of the body’s cleaning mechanisms, and especially the function of the kidneys, depend intimately on water and salt. Drink alkaline water on an empty stomach—at least 3.5 litres per day. Eat plenty of salt with all your food—at least a full teaspoon. The more you sweat, the more water, and the more salt you need. We looked in detail at how much of each is optimal in How much salt, how much water, and our amazing kidneys.
When do we eat?
If we train in a fasted state, the best is to train in the first part of the day, taking advantage of the fact that the fast has already lasted 12 hours or so. We can rather easily extend that further, and train around noon, following about 16 hours of fasting. Either way, we will want to eat between one to two hours after training, allowing a good amount of time to make sure the body is well hydrated, and stress levels have dropped. This will bring us to having our first meal of the day somewhere between 12:00 and 15:00. Different people have different schedules and preferences depending on the rhythm of their work and personal life. There are no hard rules, and things have to remain flexible, as irregularity is also an important part of training the body to be more adaptable. In fact, you should be somewhat irregular with your schedule for just this reason.
We can have only one meal per day, or we can have two, or we can have one big meal and some snacks, or, best of all, we can sometimes have one meal, sometimes two meals, sometimes have snacks, and sometimes not. The main point in training the body for optimal metabolic efficiency, is to be a significant amount of time, somewhere between 12 and 20 hours, without eating, and to train in a fasted state, in conditions of low blood sugar and low insulin levels. We discussed intermittent fasting in The crux of intermittent fasting, concluding that one of the most important points for successful and effective intermittent fasting is that the body be fuelled by fat and not by glucose. As you will have gathered by this point, our context here relies on the fact that the body is keto-adapted, and therefore, fuelled by fat.
What do we eat?
That was the original question my friend wanted answered, and it is, in a way, very simple to answer: we eat only the least contaminated, least processed, and least insulinogenic, the most natural, most nutrient dense, and most digestible.
Least contaminated means minimising our body’s exposure to toxic substances, heavy metals, hormone disruptors, pesticides, herbicides, chemical additives, anything that is toxic in one way or another. Least processed means minimising manufactured foods, of which we don’t need any. Least insulinogenic means minimising foods that stimulate the secretion of insulin from the pancreas, and this means minimising intake of simple sugars and starches, and not over-eating protein which is about half as insulinogenic as carbohydrates.
Most natural echoes least contaminated and least processed, but additionally implies a freshness, a wholesomeness, an absence of adulterations and manipulations. That’s what we want. Most nutrient dense means maximising mineral content, vitamin content, optimising amino and fatty acid profiles, and overall micronutrient content for a given amount of calories. Most digestible means minimising digestive stress, maximising enzyme content and nutrient absorption.
Digestion, the function and health of the digestive system, is essential. Everything from the food we eat is made available and usable—or not—by and through the digestive system. We have written about digestion on many occasions, but most specifically in Understanding digestion, Intensive natural healing, and Why we should drink water before meals.
But in practice, what do we eat? No junk of any kind. No polyunsaturated oils. No sweet things. No starches. Excellent animal foods and excellent plant-based foods: grass-fed, full-fat meats and organ meats like liver; nutrient dense and non-toxic fish like sardines, herring, anchovies, seafood and wild fish (avoid tuna, swordfish and any other large predatory fish, because they contain large amounts of mercury and other heavy metals); fatty nuts and seeds, especially coconut products, but also walnuts, macadamia, almonds, hazelnuts; dark leafy greens, both in salads (mixed baby greens, baby spinach, arugula, lamb’s lettuce, lettuces of all kinds) and steamed (chard, spinach, and anything similar); green vegetables like celery, cucumbers, broccoli, asparagus, and string beens; colourful vegetables like purple cabbage, red and yellow peppers. You can eat pretty much anything you can think of that is not processed, nutrient poor, or highly insulinogenic.
What should you have for breakfast? We already solved that problem! You do not eat breakfast anymore, remember?
What do you have for lunch after training? You’re in a rush or just lazy? Well, make yourself a coconut milk smoothy. You can put some protein powder (whey or plant-based, but never soy!), some superfood powders, some hemp or chia seeds. You prefer it sweet-tasting? Put some raspberries or blueberries, and stevia extract. You prefer it green and salty? Put some spinach and salt. In both cases, you can add avocado whenever you want. You can make it with cacao powder, with vanilla extract, or with almond extract. You can add raw or roasted almond or hazelnut butter, sunflower seed butter or tahini. Anything you want that is wholesome and healthful. You’ll need to experiment to find combinations you like. Start simple with few ingredients, and add things bit by bit to keep on top of the process and the blends of flavours.
If you’re not in a rush, or don’t want to have a smoothie? In this case you eat exactly as described above: healthy, nutrient dense animal and plant-based foods. This can be as simple as a can of sardines with a bag of organic baby greens. And for supper, the same as for lunch, really. The same simple and basic principles apply to everything you eat at all times, with these two additional points to keep in mind:
The first is that because we do not eat for a significant part of the day, and also because we eat either just one or two meals, it is crucial to get enough calories and fat, nutrition and protein. Otherwise, we will quickly find ourselves in calorie deficit, and this means that if we keep it up for a long time, we will first burn through our fat reserves, and then burn through our muscles. As athletes, we definitely do not want this. So, it is very important to get all the calories we need, especially if we train a hard or long hours on a daily basis.
The second is that for good, deep and comfortable, restful and restorative sleep, we shouldn’t go to bed on a full stomach, and most importantly, not on a stomach full of protein. Digestion is energy intensive. In the case of protein, it is also highly thermogenic, which means that it generates heat. Therefore, going to bed after a large protein meal will lead to a restless, tossing, turning, hot and uncomfortable sleep. For a deep and restful sleep, we want the opposite: little digestive activity, a slow heartbeat, and a low body temperature. This means that large protein meals should be had several hours before bedtime, in the afternoon or early evening, allowing a good three to five hours for full digestion before going to bed. If you can’t avoid eating late at night, then eat light: a salad is perfect. For a snack instead of a light meal, have a couple of tablespoons of almond butter on cucumber slices or with celery sticks, for example. Because sleep is really the most important part of the body’s recovery process, it is imperative to optimise sleep.
Closing thoughts
With all of what we have discussed mind, is it really any surprise that more and more professional athletes are opting for this metabolic advantage? A number of years ago, the tennis champion Novak Djokovic divulged one of his secrets. What was it? It was exactly this. This year, the third time winner of the Tour de France, Chris Froome, also divulged one of his secrets. What was it? It was exactly this. Are you curious, say, about Froome’s standard first meal of the day? Four poached eggs, smoked Alaskan salmon, and steamed spinach. Surprising breakfast? Not in the least. Indeed, an excellent breakfast!
We are seeing more and more runners, swimmers, triathletes, but also power lifters and body builders making the switch. It is to their advantage, and when they themselves feel the difference it makes, they know it to be true, at which point there is no turning back. Obviously! Who in their right mind would give up such a metabolic advantage? I suspect that eventually, this will be the standard.
And it’s not surprising at athletes from various disciplines have made these changes to their diets and lifestyles. What is surprising is that so few have actually done this. The change is low, but there is a clear shift in this direction. This is attested by witnessing training specialists promoting these principles, training athletes in this way, and demonstrating the immense advantages that it brings to them in their performances. Vespa Power discussing fat utilisation on their website is a good example.
Is all this stuff new? Of course not! Medical doctors, nutrition researchers , diabetes and metabolic medicine specialists have been talking about this for many decades. Some pioneers include Atkins, Rosedale, Volek and Phinney. And the tradition has continued and expanded, especially in the last decade.
Is this the whole story? Of course not! It never is. But it covers the basics. I plan to explore different aspects of what we started discussing here. You can read more about all these things on blogs and websites. Here are three I have read: the athletic MD Peter Attia had a good blog with many informative articles (especially in the beginning) about physical performance at different stages of his own keto adaptation process. The professional ironman triathlete Ben Greenfield also has written about his experience going form fuelling his body with glucose to using fat instead. I point to these because they have articles specifically about the process of keto adaptation we describe above as foundational for optimal sports performance, and also because they were both meticulous in quantifying the physiological changes and writing about them.
Marty Kendall has a very good blog on optimising nutrition in the sense that we have discussed here, and have been writing about for five years, starting with our very first post, What to eat: four basic rules. But what Marty has done is to actually quantify the value of foods, using the USDA nutritional database, assigning to each food an insulin index derived from its insulinogenic potential, and a nutrient density score based on its macro and micro nutrient content. The associated Facebook group is a great resource for information on this and related topics.
Now that we’ve reached the end, I hope this was useful, and that I have managed to show that, whatever the reason or motivation, whatever the sport or skill set required, there is really no other option other than this when you are serious about optimal physical performance.
If you think this article could be useful to others, please ‘Like’ and ‘Share’ it.