In What about cholesterol we saw how important cholesterol is for so many essential bodily functions and in so many important ways, that there should never have been a shadow of a doubt in anyone’s mind that cholesterol is anything but essential and vital to our health and our life. And that, therefore, it is ridiculous to even have to say that cholesterol is good for us. However, it is more than completely absurd, non-sensical, and outright dangerous to claim that it is bad for us. Let me assume you are now well convinced of this.
There is something we didn’t go into that relates to the fact that we’ve been told—and continue to be told—that we should minimise our intake of dietary cholesterol. The crazy thing about that recommendation is that the amount needed by the body of this vital substance depends solely on the body’s needs for it. And thus, the normally functioning liver, supplied with adequate amounts of the essential building blocks, produces cholesterol in the amount that is necessary for proper bodily function—whatever that amount happens to be at a particular time. What this means is that in a healthy individual, the amount of cholesterol you eat should not really affect the amount of cholesterol in the blood, estimated by the concentration of the lipoproteins that transport it to and from tissues.
Even though this obvious consequence of considering the body’s physiological function should just be accepted as a plain fact, unfortunately, most people—including health professionals—don’t. We continue to believe that cholesterol is bad, and we continue to try to minimise dietary cholesterol in order to lower lipoprotein concentrations, completely ignoring the fact that cholesterol and lipoprotein production is an exceedingly refined and well regulated mechanism that responds directly to the body’s needs.
It is certainly possible that if dietary cholesterol intake decreases, the liver produces more, and if dietary cholesterol intake increases, then the liver produces less; to what extent certainly depends on the physiological circumstances, and specific needs for cholesterol depend on many factors, all related to the state of the body. But it is pretty well established that the body produces more or less the same amount of cholesterol regardless of the dietary cholesterol intake because it much prefers to use the kind of cholesterol the liver produces, which is free or un-esterified cholesterol, rather than having to de-esterify the dietary cholesterol that comes primarily as cholesterol ester. Therefore, much of the dietary cholesterol is used in bile and excreted through the intestines.
For a lot more details, you can check out Peter Attia’s essential points to remember on his series The straight dope on cholesterol, even if I don’t really agree with the points linking LDL with atherosclerosis, simply because lipoprotein concentration, particle number, size distribution and everything else are all secondary or even further removed consequences of other dietary and metabolic factors upstream. In fact, I believe we should not even have started measuring lipoprotein concentrations and cholesterol in the first place. What we should have always focused on are uric acid levels and tracers of inflammation. And on another note, Peter is categorical that dietary cholesterol is not absorbed and all excreted. However, a couple of review papers I read about lipid absorption state that about 50% of intestinal cholesterol is, in fact, absorbed. The truth is that it is almost certainly dependent on a whole slew of factors and that, as for all things, the body absorbs and excretes in accord with its needs.
A viral infection, for example, will generally lead to the increase of lipoprotein concentration because these are the molecules that can most effectively gobble up and destroy viruses. Dehydration leads to a scarcity of water at the cellular level. As a consequence, each cell’s survival relies on producing more cholesterol in order to more effectively seal in the precious water it depends on for life that appears to be so scarce. Hence, dehydration also leads to higher cholesterol. A diet high in sugar—simple and starchy carbohydrates—naturally leads to a much greater amount of damage to cells and tissues throughout the body, but especially to the blood vessels themselves, from the highly damaging presence of insulin, the result of glycation of proteins and fats by higher concentrations of circulating glucose, and several other related factors. To repair the damaged cells, cholesterol is needed, and thus, in this case also, lipoprotein concentrations rise accordingly.
Although the fact that the amount of dietary cholesterol does not affect blood lipoprotein concentrations much is not debated by people in-the-know about issues pertaining to cholesterol, I just wanted to see this for myself what would happen. So, I devised a simple self-experiment: compare the lipoprotein concentrations in my blood when following my low-card, high-fat, high-nutrient diet, to those after eating 6 eggs per day for 6 days in a row, where I basically just added to my diet more eggs, usually raw in smoothies. That’s a lot of eggs… But before I present the results, I think it’s important to go through a few numbers relevant to this discussion.

Eggs: An average organic egg of 50 g supplies 70 calories, and contains 5 g of fat (all in the yolk), 6 g of protein (all in the egg white), less than 0.5 g of carbohydrates and 215 mg of cholesterol. This means that 6 eggs supply a total of 1300 mg of cholesterol. For me, 6 eggs per day is 3 times my usual consumption of 2 eggs per day on average—a 300% increase.
Blood volume: The blood in our body accounts for about 7% of its mass (Ref). For a weight of 100 kg, there is 7 kg of blood (about 7 litres); if you weight 50 kg, then there is 3.5 kg of blood or about 3.5 litres. And therefore, for a 57-58 kg person like me, this makes almost exactly 4 kg, and thus about 4 litres or 40 decilitres.
Lipoproteins: Cholesterol is not water-soluble, and thus has to be transported by lipoproteins. Different lipoproteins carry a different amount of cholesterol. The bulk of it, however, is found in LDL and HDL molecules. The percentage of cholesterol by weight in LDL is about 40%, and in HDL it is between 20 and 35% (Ref). To keep our calculation simple, we’ll take this to mean that LDL is half cholesterol by weight, and HDL is one quarter cholesterol.
Here are the results of the blood tests from December 16 and 22, 2011, both taken in the late afternoon after nearly 24 hours of fasting (I do this every week, so it was nothing unusual). And please don’t worry about the boldface: it appears automatically if the numbers are not in the “recommended” range, which for cholesterol is below 200 and for glucose 65-110 mg/dL. And don’t worry about the spelling: it’s spanish because I live in Spain.


Now, looking at the results, can you guess which one is which: which is the result of the blood test before one week of 6 eggs per day, and which one is after?
The answer is that the first table is from the blood test done on Dec 16, and the second table is from the blood test done on Dec 22:
After one week of eating 6 eggs per day, the LDL decreased from 110 to 95 mg/dL, the HDL increased from 106 to 112 mg/dL, the “total cholesterol” decreased from 224 to 213, and the triglycerides decreased from 41 to 29 mg/dL.
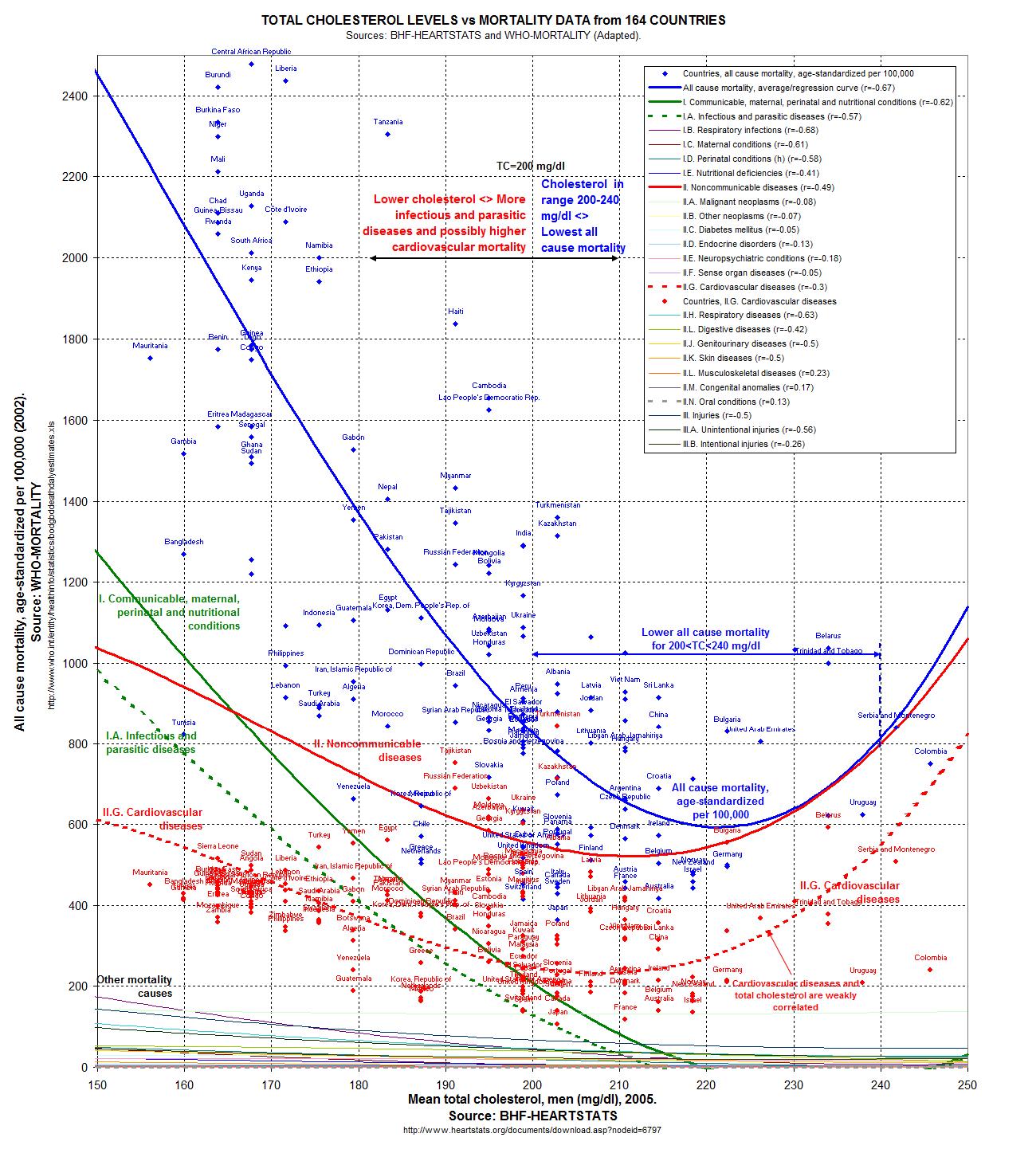
About the lipoprotein concentrations, you may recall from this graph I linked to in my first post on cholesterol, and in which was compiled all the available data found by its author, that included mortality rates and what is referred to as “total cholesterol” (but is in fact total lipoproteins), the ideal range for which is labelled “Colesterol total” in the above test results is 200-240 mg/dL, and the minimum all-cause mortality is found for concentrations of 220 mg/dL. That’s right where my numbers happen to be.
As for the glucose, well, you already know I try to keep it as low as possible, and by the way, I had no signs of hypoglycemia when my blood glucose was 60 mg/dL. In fact, I never do, even during three-day fasts, cycling to and from work, and doing resistance training at lunchtime. This demonstrates that the state of hypoglycemia can not be defined by a fixed threshold of glucose concentration below which we are considered to be in that state, but rather is based upon the individual’s metabolic function. This should be obvious since some people feel the consequence of hypoglycemia quite regularly and at glucose levels that would be exceptionally high for others, who on the contrary never feel them, simply because their metabolism has been trained to use fats for the body’s energy needs efficiently, and in fact, almost exclusively—to function in ketosis—as is my case. I plan to revisit this topic in greater detail in the future. But for now, let’s come back to the blood test results.
Firstly, we see that the sum of LDL and HDL compared to the “total cholesterol” is 216 vs. 224 (Dec 16) and 207 vs. 213 (Dec 22). This tells us that the VLDL (very low density lipoproteins) and CM (chylomicrons) together account for 8 mg/dL on Dec 16, and 6 mg/dL on Dec 22. They are, and we’ll not discuss these lipoproteins any further in this post.
Secondly, we note that the small difference in the very low concentrations of triglycerides (three fatty acids attached to a glycerol backbone), considered to be “normal” up to 150 mg/dL, mirrors the small difference in the lipoproteins that carry most of the triglycerides: the CM (90% triglycerides) and VLDL (62% triglycerides). Low triglyceride levels with low glucose and insulin levels equate to efficient metabolic use of fats.
And thirdly, we find that for 4 litres of blood, if we assume simple rounded figures of 100 mg/dL of LDL and 100 mg/dL of HDL, the total amount of cholesterol being carried around in the bloodstream is about 3000 mg: 40 dL*(50%*100 mg/dL + 25%*100 mg/dL). This is just 3 grams in the entire blood supply for a body weight of 58 kg! And an additional 1300 mg of cholesterol per day—almost half of the cholesterol in the bloodstream—from eating 6 eggs, and this for 6 consecutive days that supplied a total of 7800 mg of cholesterol, did not affect the lipoprotein concentration.
This leads us back to the hypothesis presented in the first paragraphs: the amount of cholesterol you eat should not really affect the amount of cholesterol in the blood. And although a quick experiment on a single person is far from being definitive proof of anything, this one clearly indicates, at least for me, that increasing intake of dietary cholesterol by an amount that is close to half of the total cholesterol circulating in the bloodstream, and doing this each day for 6 days in a row, does not raise lipoprotein concentrations (in this case, they went down slightly) when comparing the values measured at the same time in the late afternoon after a 24 hour fast once at the start of the week and 7 days later.
Furthermore, based on the sensible assumption that cholesterol synthesis by the liver is a response to the body’s needs, but also ability to manufacture it, if absorption of intestinal cholesterol is not nil but varies depending on the body’s needs, then supplying more dietary cholesterol may help ease the requirements on the liver for manufacturing the quantities needed. Therefore, this “help” to the liver can only be viewed as favourable considering the extreme importance of this organ for good health. It could also be that most or even all the additional dietary cholesterol was simply excreted in the stools. But in any case, it is absolutely certain that eating this huge amount of cholesterol every day did not affect lipoprotein concentrations in the blood after the period of fasting.
What I would like to do is to evaluate dietary cholesterol absorption on me, a 40-year old man in excellent health, by adopting an extreme diet of eating only eggs and water (this will remove the influence of other foods and nutrients and therefore reduce significantly the number of variables that can influence cholesterol synthesis and absorption), and take minimal blood samples at regular time intervals such as every hour or every couple of hours. By evaluating the changes in cholesterol transporters we would be able to estimate how much is absorbed because we know that lipids from the intestines are transported to the blood mostly by CM and VLDL, whereas HDL and LDL are mostly responsible for transport to and from the liver.
In any case, as we have seen here, but also as I mentioned in my opening sentences that we have known for a rather long time, dietary cholesterol does not influence blood cholesterol much. So please, when you hear someone say that we should avoid eating too much cholesterol because they have “high cholesterol”, you don’t need to say anything if you don’t want to, but remember at least this: cholesterol is so important and so good for us, that the liver and cells themselves will always do everything to supply the all the cholesterol that is needed, whatever that is at a particular time, and no matter how little or how much we get from our food. And maybe it is even the case that eating more cholesterol actually helps the liver and cells meet the body’s continuous demands throughout the day and night of this vital substance.

{kind=link}