Yesterday I had a video coaching session with one of my patrons, and the last thing we talked about was the gall bladder. They recently had an ultrasound done to check out the insides of the abdomen—obviously to make sure everything looks good. The kidneys looked good, the liver had a small benign lump of 1–2 mm in size (angioma sounds so much more serious), and the gall bladder had a bunch of little stones. I asked what the doctor recommended.
“There’s nothing to worry about. Let’s check again in half a year.” That was it. Nothing more. So, they asked me if there was anything that could be done to help in some way.
What do you think? Is there not always something that can be done to help—to help the body cleanse itself, repair itself, heal itself, improve its physiological and metabolic functions?
We’ll take the time to study and explore the liver and its functions in greater detail later—the liver is a lot more complex. The gall bladder is quite simple, and so, I just wanted to share with you what I explained yesterday, and at the same time, take the opportunity to expand a little on that.
First the Anatomy
Looking at the abdomen from the bottom of the sternum (the bone between the pectorals) to below the hips, after having removed the skin and layers of muscle, cut out the front part of the ribs, and changed the appearance to make it cartoon-like, without any blood, veins, arteries, or nerves, and thus not so shocking to look at, we would see something like this:
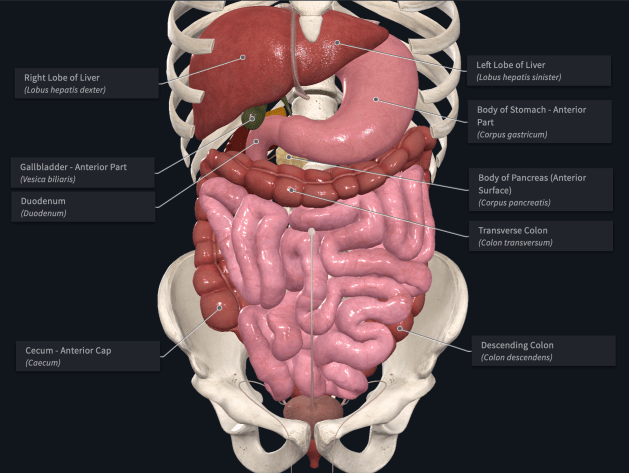
Digestive system: front view with labels
The large, dark red organ that is the liver sits at the very top of the abdomen with its largest lobe located on the right side of the body. On the left, below the liver’s smaller left lobe, is the stomach that curves back towards the middle where it connects to the small intestine (duodenum). The gallbladder—the small dark green pouch—is nestled between the bottom of the liver’s right lobe and the first part of the duodenum. Below the stomach, sweeping across the abdomen from one side of the body to the other is the transverse part of the large intestine (colon). The entire lower portion of the abdomen is filled with the longest segment of the intestines.
If we zoom in on the upper abdomen,

Upper digestive system: close up front view
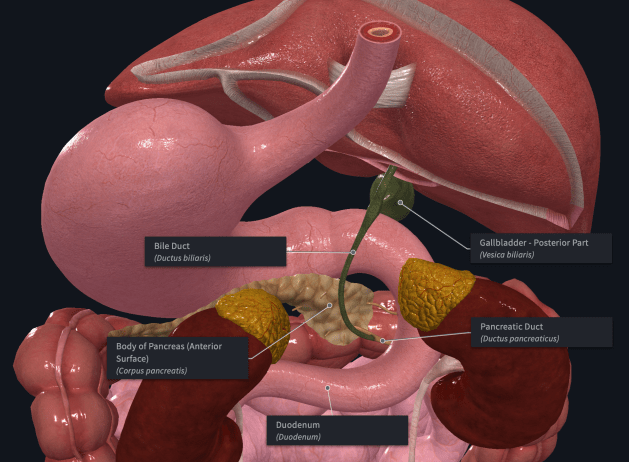
and then hide the liver,

Upper digestive system: close up front view without liver to show bile ducts
we see all of the little green ducts embedded into the liver whose function it is carry the bile from the different parts of the organ to the main bile duct and gallbladder.
Taking a look at the same part of the abdomen from the back,
Upper digestive system: close up back view with labels
we see how the gallbladder sits between the liver and duodenum, and how the main bile duct sweeps down behind the pancreas to connect to the main pancreatic duct such that the bile from the liver and gallbladder can be injected into the small intestine together with the enzymes, insulin, glucagon, and bicarbonate from the pancreas. We also see from this side the dark red, bean shaped, right and left kidneys, and the yellow adrenal glands sitting on top of them.
And then the physiology
Why do we need bile and what does it do? Why is there a gallbladder? And what is bile anyway?
Bile is 97% water, 0.7% bile salts (sodium and potassium), 0.5% cholesterol, fatty acids, and lecithin, 0.2% bilirubin, and a tiny bit of inorganic salts. In human adults the liver produces 400–800 ml of bile per day (Wikipedia).
The liver produces bile continuously but slowly. When we eat, depending on how much fat there is in the meal, the digestive system may need quite a bit of bile to handle the fat that was just ingested. Hence the need for storage and thus the function of the gallbladder.
The purpose of bile is to emulsify fat. Emulsifying means making into tiny droplets that can mix into another liquid to form a smooth homogeneous solution. For example, a bit of mustard works very well to emulsify the oil and vinegar that would otherwise not mix into a smooth creamy vinaigrette. After emulsification, fat droplets are typically 15–30 microns in size.
We need bile to emulsify the fats that we eat so that the pancreatic enzyme lipase can then break these triglycerides down into monoglycerides and free fatty acids. This is done in the small intestine where the bile and enzymes are secreted from the pancreas with the bicarbonate solution. This in turn allows the fat to be transported through the intestinal wall before being reassembled into triglycerides and absorbed into the lymphatic system. Without bile, fat could not be absorbed. It would go straight through the gut and be excreted undigested.
Why would stones form in the gallbladder? Is there a way to prevent the formation of gallstones? And what actually are these gallstones?
Gallstones are basically little hard lumps of cholesterol. One of the functions of the gallbladder is to concentrate the bile which comes in quite diluted, as we saw earlier, being 97% water. But when the concentration grows too high, then cholesterol precipitates out and forms little lumps. These are what we call gallstones.
Given that we know that stones form out of precipitated cholesterol when the concentration of the bile is too high in the gallbladder, it is simply logical that if the concentration can be kept low enough, below the threshold at which cholesterol will precipitate, then no stones would form. But why does the concentration of bile grow to the point of precipitation?
Let’s ask another question: what happens if we don’t eat much fat? The liver produces bile continuously, between 400 and 800 ml per day. This bile is stored into the gallbladder until it is needed after a meal in which fat was ingested. If we don’t eat much fat in a meal, then, naturally, not much bile will be needed, and most of the available bile will therefore remain in the gallbladder. Because the liver continues to produce it, the gallbladder needs to make room for it, and thus concentrate its contents further.
So, what happens if we never eat very much fat, and if actually, every meal is a relatively low fat meal? Well, what happens in a pool of water if the water does not flow out, and is by this not renewed by fresh water? Stagnation. In the case of the pool of water, we all know what happens: it grows dirty, then thick, then greenish, then totally filled with lumpy green gelatinous stuff. In the case of the gallbladder, we can imagine that something analogous takes place, and that the lumps of cholesterol are like the lumps of green gelatinous stuff in the water.
The solution is simple: eat plenty of fat on a regular basis. This way, the gallbladder can empty itself out regularly, and the bile does not stagnate, grow more concentrated, and eventually lumpy with gallstones.
Your gallbladder and why it’s important
Here’s what we learned:
The gallbladder sits between the right lobe of the liver and the first part of the small intestine. It stores and concentrates bile which is mostly water with small amounts of salts, bilirubin, lecithin, and cholesterol. The liver produces bile continuously in the amount of 400 to 800 ml per day.
The function of bile is to emulsify the fat we eat to make it absorbable. Without bile, fat just go through and gets excreted undigested. The same is therefore true for all fat-soluble minerals and vitamins, including some of the most important of them all, the crucial vitamins A, D, E, and K2.
If we don’t eat fat, there’s no need for bile. If we don’t eat much fat for a long time, the bile will get more and more concentrated. Eventually, the concentration will be high enough for cholesterol to precipitate out of the bile and form little lumps. These lumps of cholesterol are called gallstones.
Imagine that this continues for years and even decades, following a good “heart-healthy” low-fat diet. What do you think will eventually happen based on what we’ve just discussed? More stagnation, more highly concentrated bile, more gallstones, and then at one point, this whole thing explodes into acute infection, acute inflammation, excruciating pain, and emergency surgery to remove the infected gallbladder.
And then what? I’ll you finish this exercise in deductive reasoning which you now have all the necessary background to complete.
Thank you to all our patrons, and in particular Eric Peters and Toni, for their continued support. Become a proud sponsor of healthfully and join our patrons today!
